| Home | PLS Info | Helpful Tools | Journal | Genealogy, Stories, Photos |
|
|
|
Journal - PLS & ALS and the Challenges |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Life with an
Assistance Dog – Lynn Holmes Quixote, my ADI trained service dog, is
happiest when he is doing things for me. It’s really about how can I serve
you! And I would cherish him for his help, if that’s all Quixote did. But we are best buddies. We go everywhere
together-he stays by my side in the bedroom and bathroom, watching TV, at the hairdressers, and on long walks on bike trails. We’re inseparable. If all he did were pick up things I drop,
that would be enough. Quixote makes me relaxed about dropping things. At home, I used to spend a lot of my very limited energy trying to get things off the floor using a reacher. The hand strain alone was exhausting. Out
in the community if I dropped something I was SOL, unless someone came by and helped.
Most of all, my assistance dog is an energy saver and a big confidence builder. As a team, we’ve figured out ways
for Quixote to understand what few words I can speak and what my various mumbles mean.
You see, PLS (primary lateral sclerosis), has left me unable speak clearly, as well as affecting my mobility. My voice was my livelihood, as an attorney and sales person. Having no one understand my words was demoralizing. I just
wanted to crawl in a hole. Then along came Quixote! Wonder Dog! He understands me!
What a fantastic feeling! And he does everything I ask of him. Sometimes we get creative, like flipping a light switch: A
couple switches don’t have space for Quixote’s paws on the wall, so I position myself so he can use my lap to
stand on, then Quixote leans over and flips the switch. Now I go outdoors nearly everyday. People approach Quixote, often stopping to chat with Quixote and me. Cashiers light up when he pays! We go all over Santa Rosa,
just the two of us-on the bike trails, on the bus, to the mall, to the movies, and to the parks. One of our first
outings was to my nephew’s high school baseball game. At the end of an
inning with all the cheering and high 5’s on the field, Quixote, being the ultimate people dog, had to join in. Quixote bolted and I dropped the leash. In
a split second, there he was, on the pitchers mound, surrounded by boys. I beeped
my horn on the wheelchair and he returned, happy as could be! ADI will ask you in
the months to come, if your dog is beginning to know what you’re thinking. And
yes, your dog will anticipate your needs, but I think the more important question is:
Do you know what your dog is thinking? With Quixote, around
10pm he looks at me saying with droopy eyes, asking why aren’t we in bed? Yes,
he starts out sleeping in my single bed, under the covers, snuggled up close to me.
As my partner, Quixote
helps me with many daily chores. He ·Opens and closes doors ·Gets clothes I point to from the closet or a drawer ·Flips light switches ·Opens the refrigerator and closes it ·Speaks when I click a dog trainer ·Opens and closes the pantry door and if it’s time gets
his daily bag of his food, he places it in my lap ·Picks up anything I drop ·Pays cashiers ·Just this week Quixote learned to take my jacket off me (followed
by cheering and many kisses.) · Knows my eyeglasses and TV remote don’t belong on
the floor and Quixote gets them and brings to me ·And, knows I don’t belong on the floor! My agency sent a new caregiver and she did well, until it was time to transfer me back to my wheelchair. I ended up lying on the floor and Quixote just calmly placed himself between the caregiver
and me. No aggression. No barking. Just a calm demeanor, but positioned to say, “Ok you’re not touching my
person again.” Quixote moved when the paramedics came and when everyone
left, we had a lick-fest. About the lick-fest
- I think I’m his favorite toy. You see, Quixote is a lick monster! He loves to stand on my footrests and lick me all over my face, head and hair. He goes nuts. I’m amazed at how
long he can stand on his hind legs. I cry uncle long before he’s ready
to stop the sloppy kisses. As each of you will
find, an assistance dog from ADI is only a small portion of what ADI provides. ADI
has given me more than a service dog; they’ve given me partner who has restored my independence and confidence.
Nutritional Information Each
Ounce of Ultra Body Toddy™ provides : *
Daily value not established
Yahoo!
Medicare paid for my seat elevator: Several
points to keep in mind:
As many of you know I have Primary Lateral Sclerosis (PLS).
PLS is a rare disease similar to ALS-Lou Gehrig's Disease. PLS slowly paralyzes the limbs, affects the ability to speak, but
does not affect thinking. PLS does affect the way I live day to day, but should not shorten my life span. This disorder slowly damages the nerves that help me walk, speak
and use my hands. PLS is progressive, and will make it more difficult for me as time goes on. However, I hold on to a positive
attitude and make the best of everything life places before me because there is so much to be grateful for. Although
there is currently no cure, I have a lot of hope because research is finally accelerating. Experts are hopeful that cures
can be found in this generation. My sister and her husband really have made living with PLS (Primary Lateral
Sclerosis) bearable. Their 2 children also help me everyday and by taking all the physical changes without any negative judgments.
I'm still the Aunt who spoils them. In 1999 I had some numbness in my left foot when I'd walk along the beach.
I figured my shoe was to tight, after all I'd gained a little weight. I ignored the feeling. Then 2000 I moved north
to practice law and when jogging with my sister she notice my left foot was dropping in a funny way. Well, one doctor
exam lead to another and one referral end in many referrals. One test lead to so many tests, x-rays and scans I almost lost
track. I got into University of California San Francisco Medical Centers and saw one the top rated and very personable neurologists.
He diagnosed PLS. I still visit UCSF Medical Centers ALS Center (ALS is the closest thing they have to PLS) every 4 months.
Unlike Multiple Sclerosis, I have no pain caused by PLS. Of course falling over does cause pain. PLS effects the signals from
the brain that control the muscles of the legs, arms, hands and voice. Unlike ALS, PLS does not effect the lung or heart muscles.
So, PLS changes the way I live my life, but doesn't shorten my lifespan. PLS has one symptom that I take extra drugs for: uncontrollable or inappropriate
laughing. Sometimes the smallest thing will set me laughing (running over my sisters toe or a joke) and I laugh long and loud,
snorts and all. I guess laughing beats the other side of this symptom - uncontrollable sobbing & crying. Laughing out
loud and often. PLS is progressive and I've moved from the cane, to a walker, to a walker
& manual wheelchair to a Power Wheelchair. Battery operated (no pollution) with a 20 mile range and a top speed of 5 miles,
I zoom around. I was like a pinball bouncing off walls, through door jams and pinging off furniture while I got used to the
joystick controls. I only ran over my sister's toes twice, cats tail once and got stuck in soft sand once. When I no longer could get up and down with ease or without falling over,
I hired the housekeeper I always dreamed of. I have a caregiver who helps me save my energy for fun things. I've
learned patience. I let others spend their energy doing the endless everyday little things, so I can conserve my energy
for the important things - Having enough energy to participate actively in the lives of my family. I still manage to go to my nephew's baseball games and now football games.
My Uncle Raul found a wheelchair assessable van on EBay, which I bought. I no longer have a law practice, but since the doctors visits are now less
frequent and the PLS muscle stiffness is under control (love those muscle relaxing (medicines) I may start to write some legal
articles. I'm also finishing my family genealogy (I have 35 1st cousins on my mother's side). I'm able to order everything
from groceries to medications over the Internet. So I'm still living independently as much as possible. You know that side
of me!
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
March 2005 - I had an appointment at
the ALS Clinic. My breathing improved, I lost 7 pounds (YEAH), and I generally doing well. We think the botox
in the vocal cords helped me take a bigger breath in because I wasn't struggling to get the vocal cords out of the way. I
saw the botox speech doctor. I had botox injected into my tongue. It's not nearly as awful or painful as it sounds. My tongue
responded well but now I have difficulty swallowing. I'm taking all my food through my stomach feeding tube. I have a liquid
called Jevity. It's like Ensure but with more calories. Although, the mash potatoes from KFC (Across the street) went down
just fine. I had a botox injection on both sides of the base of tongue on Friday, March 4, 2005. By Sunday, March 6 I was
having some difficulty swallowing, or more precisely getting things from the my mouth past the back of the tongue and into
the throat for swallowing. I also had trouble using a straw. I just couldn't seem to get enough sucking power.
My speech didn't improve after the treatment.
While my tongue feels less bulky, and rises and the tip curls up more easily to the roof of the mouth, my ability to speak
has diminished. I feel my speech is less understandable and I am less able to string words together. My speech and breathing
seem to compete when I try to speak, leaving me tired. My mouth, vocal cords and tongue just seem to reach exhaustion after
I try 3 or 4 words and then I get very little volume as well as garbled, slurred, unrecognizable sounds.
It is all so clear in my mind, that I can't
believe I can't get it out! Frustrating but I'll just use the computer for speaking.
I'm still pretty much in the same state.
I'm able to eat orally foods about the consistency of custards and mash potatoes (With gravy, of course.) Yoplait custard
style yogurt works well and I use a spoonful to help my two pills a day go down. When I don't want yogurt, I crush the pills
and with water, ingest them through the PEG Tube. I am getting 99% of my nourishment from Jevity - 4 or 5 cans per day. As
before the tongue injection, I get all my hydration through the PEG tube - 50+ ounces a day. I have more saliva then before
the tongue injection. However, it is manageable without medication. I am not drooling and able to swallow the saliva. Spitting
is not possible.
My mouth and vocal cords, which were treated
with botox on Nov 19, 2004, remain well and the spasticity has not increased to become noticeable again, yet.
July 2004 - Baclofen Pump
Practitioners from around the country who have extensive experience in
intrathecal baclofen (ITB) therapy gathered in early 2004 to develop best-practice guidelines for ITB therapy. Discussion
focused on the idea that ITB therapy is a program rather than a procedure. Key recommendations were made in areas including
team coordination, patient selection and goals, patient education, patient screening, implant technique, long-term management,
individualized dosing options, ongoing evaluation of patient response, appraisal of the integrity of the catheter and infusion
system, and appropriate practice resources. Intrathecal baclofen (ITB) therapy has been shown to benefit patients with
severe spasticity related to spinal cord injury, multiple sclerosis (MS), cerebral palsy (CP), brain injury, and stroke (Albright
et al., 2003; Meythaler, Guin-Renfroe, Brunner, & Hadley, 2001; Ordia, Fischer, Adamski, Chagnon, & Spatz, 2002).
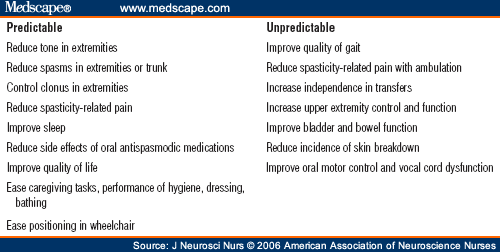
Possible outcomes vary greatly, based on the underlying neurological level of function, but may include improved ambulation
or wheelchair seating, reduced spasticity-related pain, improved sleep, and easier positioning and caregiving (Azouvi et al.,
1996; Gianino, York, Paice, & Shott, 1998; Stempien & Tsai, 2000). Documented complications occur in 10%–45%
of patients; they may include catheter disconnections, kinks, or wound infections. Acute withdrawal syndrome is also possible
but rare. (Campbell et al., 2002; Follet et al., 2003; Rawlins, 2004). ITB therapy gained U.S. Food and Drug Administration (FDA) approval for
managing severe spasticity of spinal origin in 1992 and for severe spasticity of cerebral origin in 1996. Adult and pediatric
patients may receive ITB therapy in a variety of settings, including university medical centers, community hospitals, and
private practices. In March 2004, 14 practitioners with experience in ITB therapy met in Minneapolis
to develop best-practice guidelines for providers. Participants included physicians from specialties such as neurosurgery,
neurology, and physical medicine, as well as four advanced practice nurses from around the country. This article presents
the perspective of two of the nurses and summarizes what the authors believe to be the most important recommendations from
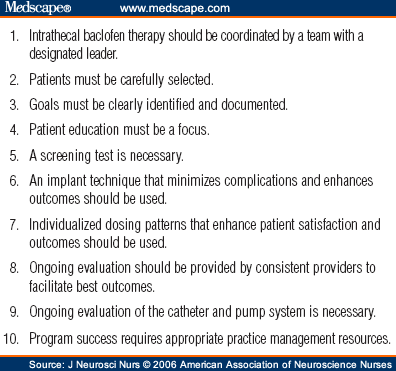
the meeting, with particular emphasis on nursing implications (Fig 1). The goal of this article is to offer practical considerations
for clinicians based on the discussions at the forum and the professional experiences of the authors. The forum took place
a few months before the release of a new pump model, the SynchroMed II ®; references to use of the new model reflect
the opinions of the authors, not those of the forum as a whole.
Top 10 recommendations for an intrathecal baclofen therapy program Successful management of patients who receive ITB therapy requires a committed
team with designated medical leadership and an identified coordinator to ensure smooth transition between the different stages
of the therapy and effective long-term follow-up. Physician leadership is usually provided by a neurologist or physiatrist
who has a focus on function and quality-of-life outcomes and a commitment to maintaining a long-term relationship with these
patients. The role of the team coordinator is best suited to an advanced practice nurse with critical analysis skills, such
as a nurse practitioner or clinical nurse specialist, who can address ongoing patient and family educational needs and ensure
that comprehensive follow-up progresses smoothly. Rehabilitation therapists, particularly from physical therapy and occupational
therapy, are essential team members who can help monitor the patient's response to treatment and changing functional status
over time. The team must make arrangements for continuous emergency coverage related to pumps and must develop mechanisms
for effective communication with clinical partners in other areas, including the primary care physician, emergency department
staff, and providers from school programs, day centers, or group homes. As with any program, experience and volume increase the competence of the
clinicians and therefore reduce the rate of complications and improve outcomes. This is a particularly important consideration
with respect to the implanting surgeon's surgical experience. However, a successful ITB therapy program involves more than
an experienced surgeon. The surgeon should be actively involved with the team for system-related problem solving and be willing
to participate in quarterly or biannual team meetings to review outcomes. The team coordinator should ensure that mechanisms are in place to provide
adequate training for all staff through competency testing and annual review, as necessary. It is particularly valuable to
review data on complications with all team members, including the implanting surgeon, as part of ongoing quality improvement
activities. To qualify as a candidate for ITB therapy, a patient must have hypertonicity
related to spasticity of cerebral or spinal origin that causes significant impairment and is unresponsive to more conservative
treatment (e.g., oral medications, local injection therapy, physical modalities). The patient, family members, caretakers,
and healthcare providers must agree that spasticity is a significant problem negatively affecting function and that treatment
is indicated. The only contraindication for Lioresal® ITB therapy for a patient
with significant spasticity is an allergy to baclofen, which rarely occurs. Adverse effects such as drowsiness, lethargy,
nausea, or mental clouding with oral baclofen are common side effects not to be confused with an allergic reaction and are
good criteria for ITB because the intrathecal delivery minimizes these side effects (Laborde, Weibel, Meythaler, & Narayan,
1999). Several relative considerations for ITB therapy have been identified, however, and appropriate patient selection involves
a comprehensive assessment of more than just the physical aspects of spasticity. Relative considerations for ITB therapy include untreated hydrocephalus,
which could impede intrathecal drug absorption and increase the risk of cerebrospinal fluid leaks around the catheter (Albright,
Ferson, & Carlos, 2005; Gilmartin et al., 2000); general medical instability; poorly controlled seizures; and severe depression,
which may be exacerbated by ITB (Ivanhoe, Tilton, & Francisco, 2001). Other concerns include a history of poor compliance
in keeping medical appointments, inadequate family or other social support, and financial barriers such as inadequate insurance
coverage or inability to take time off work to attend appointments, especially if long travel distances are involved. Patients
should be carefully evaluated to determine whether or how much they need their spasticity to maintain trunk balance, walk,
or transfer. Physical assessment should also include evaluation for an adequate body mass and abdominal girth to support the
pump. The patient and family need to understand the time required for each stage
of therapy; the need, in most cases, for physical or occupational therapy to maximize the benefits; the long-term commitment;
and the costs involved in returning to the center for dose adjustments and pump refills. A social worker's involvement is
often beneficial to address issues related to insurance coverage and transportation. Some centers develop a contract for the
patient, a family member, or caregiver to sign. Unrealistic expectations must also be addressed at the patient-selection
stage to avoid pitfalls later on. Providers must be clear with a patient with MS, for example, that ITB therapy is a treatment
for the symptom of spasticity, not for the underlying disease. A young, ambulatory patient who has had a traumatic brain injury
must understand that the baclofen pump may substantially improve his gait but is unlikely to return him to his pre-injury
level of physical agility or mental function. Referring a patient who is considering ITB therapy to another patient who
has the pump is often helpful for peer support. Care must be taken, however, to not unwittingly promote unrealistic expectations
by having a nonambulatory spinal cord–injured patient, for example, talk with a stroke survivor who can now walk without
a cane. Large centers can usually find a good peer match, in terms of diagnosis and functional level, from within their own
caseloads. Medtronic—the manufacturer of the SynchroMeddd® pump—has an ambassador program that can
be of great value for smaller facilities or those just establishing their program. Patient and family education must start in the screening phase and continue
throughout the program ( Table 1 ). Brochures, videotapes, and DVDs are available. A sample pump should be
demonstrated to the patient during the selection stage to avoid any future surprises. Even the SynchroMed II pump, with its
slimmer profile, is quite large, at 7 cm in diameter. Most patients, even young children or very small adults, tolerate the
presence of the pump without problems once it is implanted, but concerns related to the pump's appearance and sensation should
be addressed in the screening. Patients may be reassured by seeing or talking with another patient about this issue or by
holding a demonstration pump in their waistband during an office visit. The goals of therapy must be clearly identified in advance and individualized
for each patient. Goals may range from improving gait to facilitating positioning in a wheelchair, controlling spasticity
without drows1ness, controlling mental clouding from oral medications, improving oral motor control, or allowing caregivers
to perform hygiene or bladder-management tasks (Azouvi et al., 1996; Bjornson et al., 2003; Meythaler, et al., 2001). Possible
goals are summarized in Table 2 . Discussion of the goals of ITB should include consideration of the need
for physical therapy to help build muscle strength and facilitate new motor learning if the patient is using his or her spasticity
for some functional benefit, such as transfers, trunk balance, or ambulation. Goals need to be realistic, have clearly identified time frames, and be
developed with input from the patient, family, caregivers, and team members such as physical, occupational, or speech therapists
in the institution, community, or school setting. It can be valuable to have the patient or a family member sign a modified
consent form that includes the agreed-upon goals or, if feasible, to document the agreement of goals on videotape. Goals may need to be modified as the patient progresses through the stages
of ITB therapy. As response to the treatment is evaluated, outcomes and revised goals should be documented. The use of a validated
tool to measure goal attainment is highly desirable, but because goals vary greatly, depending on underlying disability and
level of function, identifying one tool to adequately address all patient situations is challenging (Pierson, 1997). The Functional
Independence Measure (FIM™), the Short Form 36® (SF-36), the Gross Motor Function Classification System (GMFCS),
and the Pediatric Evaluation of Disability Inventory (PEDI) are suggested, but all have 3. Goals Must Be Clearly Identified
and Documented. limitations. Rehabilitation disciplines such as physical, occupational, and speech therapy can also offer
specific outcome tools. One measure that may be appropriate in a wide variety of situations is the Canadian Occupational Performance
Measure© (COPM), which allows patients to rate their own performance and satisfaction with goal achievement in
three domains: self-care, productivity, and leisure (Carswell at al., 2004). Success with ITB depends heavily on detailed patient and family education
through every stage of the treatment, from patient selection through long-term management ( Table 1 ). The patient, family members, and other caregivers must be active partners
in the therapy to enhance their satisfaction, maximize their response, and prevent unnecessary after-hour calls. Many centers
use a checklist to ensure that the key elements are addressed. Education is an important part of the patient-selection process. It includes
the need to clarify goals and expectations, explain the stages of ITB therapy and the commitment involved, and answer all
questions about the procedure. This process can last for weeks or even months in some cases, as patients try to make a decision
about this elective, invasive procedure. Patient and family education to prepare for the screening test requires
review of many of the issues addressed in the patient-selection stage, with particular emphasis on what to expect in the screening
procedure itself. Medtronic has videotapes and DVDs that describe the procedure and the goals. They are available in both
adult and pediatric versions, and some are now available in Spanish. Additional patient teaching materials are available on
the clinician Web site at www.medtron icconnect.com. These are valuable tools but need to be supplemented with individualized
attention to the specific needs of each patient. The screening test is more successful if the patient and family are well
prepared with realistic expectations. Before the implantation surgery, education needs to address the plan for
initiating ITB therapy and gradually tapering off of oral antispasmodic agents, in addition to the usual preoperative instructions.
After surgery, the patient and family should receive written information about the device model, serial number, and catheter
type and length. Patients should be encouraged to start an ITB file at home, where they will keep all relevant documentation.
They will receive a wallet-sized emergency information card, which they should be instructed to carry at all times. This card,
provided by Medtronic, contains important information for providers who may be unfamiliar with ITB therapy but may be called
upon to treat patients with symptoms of overdose, drug withdrawal, or another emergent medical problem. During ongoing management of patients with ITB therapy, education will
continue to play a key role. Issues that need to be regularly addressed and reviewed include monitoring of response to treatment,
potential complications with dose changes, and interactions with alcohol and other prescription medications. The advanced
practice nurse should periodically review issues related to ITB drug withdrawal and overdose. Initiating, discontinuing, or
changing doses of medications, such as seizure medications or selective serotonin reuptake inhibitors, may alter the response
to ITB therapy, and patients must understand the need to keep all providers informed of any medication change. Patients, family
members, and caregivers must also understand how to recognize and minimize irritants that may contribute to increased spasticity,
such as urinary tract infection, constipation, skin breakdown, or poor positioning, to avoid unnecessary or inappropriate
requests for ITB rate increases. In some cases, the patient's local primary care provider may need guidance on how to triage
for and treat causes of increased tone, instead of simply treating the symptom of increased spasticity. Patients and families need information about how their device interacts
with other technology in the environment. They can be assured that the pump will not be affected by microwave ovens, televisions,
or computers. The pump may, however, set off metal detectors at security checkpoints, for example; this will not affect the
infusion of medication, but patients should carry their ITB-therapy identification card to avoid difficulties. Patients can
also be advised to carry a MedicAlert® bracelet. MRI can be safely performed on a patient with an implanted infusion pump.
The pump will stop infusion for the duration of the MRI procedure and will automatically resume normal functioning afterward.
Precautions must be taken by the MRI technician. A 24-hour technical support department at Medtronic (800/707-0933) provides
assistance to MRI facilities. Medtronic also provides written technical information that can be faxed to radiology departments.
Patients should be informed of this resource so they can share the information with providers. Patients selected as appropriate candidates for ITB require a screening
test to confirm that they will benefit from the therapy. The screening test involves a bolus intrathecal injection of baclofen
administered by lumbar puncture. The patient's response is monitored for an 8-hour period following the procedure. A few circumstances
(e.g., the patient has a fused spine) may indicate implantation without a screening test. Performing the screening test, however,
can provide useful information about future dose, response patterns, and potential functional outcomes, which can help those
providing ongoing management after the pump is placed and can provide justification for third-party payers. A screening test
is the standard of care. The screening test may be performed in an inpatient or outpatient setting.
Emergency treatment should be readily available in the event of serious adverse reactions, particularly severe respiratory
depression. Conscious sedation may be necessary for young children or others with severe movement disorders. The screening test is more likely to proceed smoothly if an advanced practice
nurse has responsibility for overall coordination and patient and family education throughout the process. Clear communication
is particularly important if one provider selects the patient and another performs the screening test. The goals for each
patient should be clearly communicated. Before the screening test, the patient is tapered from anticoagulation medications,
if necessary, and baseline spasticity is assessed. There is no need to taper oral antispasmodic medications before the screening
test. Other issues that need to be considered include transportation; prior authorization, if required; and informed consent
by a proxy if the patient is unable to consent. A checklist is helpful. The standard dose of intrathecal baclofen for the screening test is a 50-mcg
bolus. We emphasize that this is a one-size-fits-all dose to assess the patient's general response. It is important to explain
that, after the pump is implanted, the dose will be adjusted over several months until the most effective level is determined.
The provider may vary the screening test dose in certain clinical situations to improve the patient's subjective experience.
It may be difficult to convince a patient who becomes extremely hypotonic that this response is dose dependent. Ambulatory
patients with MS are particularly likely to become too hypotonic with the standard 50mcg dose and may benefit from a lower
dose of 25 mcg and monitoring for peak effect to occur earlier than with other patients. Nonambulatory patients with significant
hypertonia or those with a combination of spasticity and severe dystonia may require a 75-mcg or 100-mcg dose to produce effect. Although some providers are doing the baclofen screening test with a continuous
infusion, this is an off-label use that is not recommended. Screening with continuous infusion does not in itself allow one
to more accurately predict eventual functional outcomes because of the likely presence of underlying weakness and the need
for physical therapy services and new motor learning to maximize the response. The lumbar puncture is performed in the routine manner; experts recommend
that opening pressure be obtained to rule out any undetected hydrocephalus. Following the injection, the patient should lie
flat for 2 hours to reduce the risk of a spinal headache but may then be up as tolerated and on the usual diet. Postprocedure
monitoring should include vital signs (especially blood pressure, pulse, and respiration) every 15 minutes for 2–4 hours,
with continuous pulse oximetry. A neurologically trained physical therapist should be available to evaluate changes in spasticity
throughout the day. The medication typically begins to take effect within 2 hours, peaks at
about 4 hours, and then gradually wears off until the patient returns to baseline after approximately 8 hours. The effect
on the patient's spasticity is usually measured every 2 hours using the Ashworth scale; a 1- to 2-point drop in key muscle
groups indicates a positive response. However, depending on the patient's presenting complaints, functional level, and goals
for ITB therapy identified in the selection process, it may also be appropriate to include other variables in the assessment
(e.g., pain level, sitting tolerance, transfer ability, timed gait) and to use these changes as a measure of a positive response
in addition to the Ashworth scores. A preprinted set of standing orders and a designated documentation tool
simplify the process and ensure that all elements are addressed. Documentation should include the baseline assessment of tone,
spasms, reflexes, and pain. The goals for the patient, the time and size of bolus dose, and the time to peak onset and return
to baseline should also be documented. Videotaping the response to record the before-and-after effect can provide an invaluable
tool for later evaluation and is recommended. At 4–6 hours after injection, the physician or advanced practice nurse
should review the response with the patient and family, including a discussion of the patient's experience. If the screening test is done as an outpatient procedure, and if the patient
remains very hypotonic after 8 hours with a delayed return to baseline, it may be necessary to consider hospital admission
if some tone is required for the patient to perform activities of daily living or transfers. Most patients can go home after
8 hours without problems and with instructions to resume oral antispasmodic medications as usual later that evening. Advise
patients to avoid strenuous activities for a few days, to drink plenty of fluids, and to stay lying flat if they experience
a spinal headache. The attendees of the best practice forum in 2004 agreed the intrathecal
baclofen delivery system is reliable. They noted that improvements in the ITB system, such as catheter connectors and durability,
have reduced the complication rate over time, primarily by reducing catheter kinking and leaking. However, the implanting
physician's experience is the most important factor in preventing immediate postoperative complications and problems with
long-term system integrity. One of the most common surgical complications is infection. The infection rate for the infusion
pump and catheter implant should not be higher than the infection rate for shunt procedures. Specific infection prevention
standards and implant methods for best outcome have been published (Albright, Turner, & Pattisapu, 2006; Follett et al.,
2004). Nursing care also contributes to implant success. Discussion of pump size
with the patient, family, and surgical team provides valuable information. The newest pump models are available with 20-ml
or 40-ml reservoir volumes. Anticipated dosing needs, patient size, and patient habits should be considered when choosing
the pump model and reservoir volume. A nurse's experience with ITB therapy contributes to successfully predicting dosing requirements,
which provides guidance in pump selection. If a high dose is anticipated or the patient lives far from the clinic, the use
of the 40-ml reservoir should be encouraged. Pump size is important in pediatric patients to reduce the risk of skin breakdown
from pump erosion. Currently planned or potential apparatus (e.g., wheelchair seatbelts, lateral
supports, suprapubic catheters, shunts, feeding tubes) should be considered in deciding on the best placement for the pump
and catheter. For instance, if a left upper abdominal quadrant feeding tube placement is expected in the future, implant of
the infusion pump on the right side and tunneling of the catheter away from potential surgical sites should be encouraged. The nurse coordinator should initiate team discussion about the spinal
level of the catheter tip to improve therapeutic outcome. Presence of upper extremity spasticity indicates the need for higher
placement. High-thoracic or low-cervical catheter tip placement is beneficial for upper extremity spasticity relief and poses
no known added risk. Although the pump is routinely replaced at the end of the battery life,
the catheter is replaced only if there are signs of decreased cerebrospinal fluid flow or catheter deterioration or if the
catheter-tip location is too low. A review of therapy effectiveness with the patient and with those providing long-term management
is important to anticipate the need for catheter replacement. If the intrathecal catheter is replaced with one at a higher
level, decreasing the dose to avoid complications of high-dose effect should be considered. If any portion of a catheter has been replaced due to questionable integrity
or flow, the initial postoperative intrathecal dose should be decreased in accordance with intraoperative findings. A dislodged
or broken catheter or a defect large enough to allow cerebrospinal fluid flow through the defect implies that little, if any,
baclofen was infusing to the catheter tip. The programmed infusion should be decreased to the initial implant dose of 50 mcg–100
mcg per day in simple infusion mode. Conservative adjustments and close patient observation determine the appropriate dose
and should mimic the initial titration-dosing phase. Current implant technique includes documentation of catheter-tip level
by intraoperative fluoroscopy or postoperative X ray. Relevant information should be communicated to the providers of long-term
therapy management. Catheter model, total catheter length, and catheter volume are crucial information to prevent high- or
low-dosing complications at later stages; this is especially true for bridge bolus calculation and system assessment during
dye studies. Documentation of catheter attachment accessories, as well as connection and anchoring technique, assist in evaluating
system complications. The SynchroMed II pump software simplifies the process by allowing implant data and notes to be recorded
and stored directly in the pump's memory. Proper implant technique during initial system placement and routine end-of-battery
pump replacement minimizes complications and enhances outcomes. The nurse coordinator contributes to implant success and decreased
complications by discussing with the health-care team crucial information related to pump size and reservoir volume, location
of implant, specifics of implanted equipment, and dosing adjustments. The nurse coordinator is the communication link between
the family, community, and hospital team. After implant, a period of more frequent visits is common during the titration
phase. The titration phase is generally defined as the time it takes to achieve a steady dose for 4–6 weeks.
These visits include slow, closely monitored dose adjustments, evaluation of positive and negative therapy effects, tapering
of oral medications, and initiation of rehabilitation services. The titration phase may last weeks or months, depending on
a number of factors. One influence is the patient's diagnosis. Those with static conditions such as anoxic brain injury may
quickly reach adequate dosing, whereas those with progressive disorders such as MS require more time—perhaps 6–9
months. Another factor is the patient's sensitivity to dosage changes. Ambulatory patients are more sensitive to rate increases
and may tolerate only a 3%–6% increase in the total daily dose. Patients receiving ITB for care and comfort may easily
tolerate increases of 10% of their daily dose (Rawlins, 2004). A patient's response during the screening test is generally a fair indicator
of the response to rate changes during the titration phase. A rapid or long-lasting screening dose effect indicates the need
for conservative dose increases. Other factors include the number and dose of correlated oral medications that will be tapered
and clinic accessibility. Appropriate dosing during the titration phase prevents loss of function and provides relief from
severe spasticity. Long-term maintenance visits for rate adjustment and refills should take
place every 1–6 months. More frequent rate adjustments are common for young patients experiencing growth spurts, patients
with progressive diseases or spasticity influenced by environmental changes such as weather, and those having orthopedic surgical
procedures. Refill frequency is a factor of dose, pump model, drug stability, reservoir volume, and drug concentration. Lioresal
Intrathecal is approved for as long as 6 months in the SynchroMed II system. During the titration phase, the simple continuous-infusion delivery mode
is most commonly employed. However, once a steady dose or definite pattern of tone throughout the day is identified, various
infusion modes can be easily programmed. This flexibility is one of the major advantages of ITB therapy. New programming options
have replaced complex continuous and periodic bolus with flex-infusion modes, with additional options for altering dosing
by day of week. Flexible dosing for workweek and weekend schedules, days with therapy, home health care, or other activities
promises to provide even more individualization. A number of programming options are available to individualize ITB dosing
for patients with changing needs (Kolaski, 2005). The use of various dosing patterns is usually based on the practitioner's
level of experience and the particular practice population. For instance, patients with spinal cord injury usually achieve
goals with a steady daily dose. Patients with MS may require a higher dose at night to prevent spasms and a lower dose during
the day to facilitate transfers. Unless periodic-bolus programming is employed, more than 3–4 daily rate changes are
rarely useful. Periodic bolus programing is beneficial for those with low catheter-tip placement who need more benefit in
the upper extremities and is an option for those with severe hypertonia. Periodic boluses are usually programmed to infuse
every 2–4 hours. In some instances, a once-daily bolus provides the relief needed to achieve the full effect of physical
therapy or ease spasticity for bathing and dressing. Generally, the bolus is programmed to infuse 1–3 hours before its
effect is desired. Technical support for these programming options is available through the manufacturer's dedicated phone
line. A wide range of total daily doses (50 mcg–1,500 mcg per day) is used
to meet the variety of patients' needs. The daily dose varies with diagnosis, function, and severity of symptoms. Ambulatory
patients require lower doses on average than immobile or bedridden patients. Patients with MS usually require lower doses
than those with spinal cord injury or traumatic or anoxic brain injuries. Patients with CP and stroke tend to have midrange
doses. One last issue is the use of commercially available Lioresal versus pharmacy-compounded
solution. Refill kits with Lioresal solution are commercially available in 500-mcg and 2,000-mcg concentrations. Some clinicians
contract with private pharmacies to compound up to a 4,000 mcg/ml solution or to mix solutions with other drugs. Many institutional
guidelines prohibit the use of compounded drugs. However, if this option is used, discussion with the patient should include
potential risks, including variability in drug strength and the effect on the pump manufacturer's warranty. The forum made
no formal recommendation on this practice. The FDA offers a report on compounded drugs (FDA, 2003). Individualizing ITB dosage takes time and requires input from other health-team
members, the patient, the family, and caregivers. Because of regular patient contact, the ITB-therapy nurse coordinator has
a unique opportunity to develop rapport with patients and families. This allows teaching the importance of patient and family
attention to subtle physical changes and the effect of environment and emotions on spasticity to identify patterns of response.
Use of dedicated patient notebooks or journals to track such changes is encouraged because it facilitates dose adjustments
and specific programming to enhance individual satisfaction and positive effects of therapy. Consistency of healthcare providers is ideal in nearly every healthcare
situation but is especially crucial to care of those with chronic conditions. It allows early identification of changes in
a patient's condition and appropriate changes in therapy management. For patients receiving ITB therapy, outcomes and identification
of potential complicating factors may be influenced by patterns recognized over time. Determination of subtle changes is dependent
on accurate documentation and corroboration among team members. The team must include the primary care provider and community
contacts such as school therapists or home health providers. The nurse coordinator is frequently in an ideal position to collect
and disseminate relevant data among team members. The forum participants described ITB therapy as a program, not simply a
procedure. Comprehensive ITB centers provide a full-service program not possible in small practices with only a few patients.
Treatment in high-volume programs not only discourages patients from doctor shopping after implant or going from one private
provider to another for refills but also enhances competency of the team through increased experience. However, this option
may not be available to all patients who need the therapy. When patients or healthcare providers relocate, or pediatric patients
graduate to adult healthcare providers, steps must be taken to communicate key information, such as catheter length, baseline
function, and goals, to ensure continuity of care. During clinic visits, the core team that manages pump refills and dose
adjustments documents procedure-related facts. Caregivers and community-based providers can also provide data on standardized
forms to help fine-tune the baclofen dose. Information from caregivers also contributes to goal attainment and gives clues
for needed adjustments in current equipment or addition of assistive devices. For instance, a wheelchair-dependent student
may experience a slow, subtle decrease in trunk tone as the ITB dose is titrated. Simple adjustments in the seating system,
such as adding lateral supports, may compensate for the new posture. This may be preferred to decreasing the ITB dose, especially
if reduced extremity spasticity achieves goals such as ease of care and improved comfort. Such needs are difficult to determine
during a clinic visit. They become apparent when the extended team is encouraged to provide discriminating input. The documented effect of past ITB dose changes, dose-dependent side effects,
and bolus infusions are the best guide to future dose changes and contribute to early identification of decreased benefit
of ITB. For example, a 10% increase in daytime dose may prevent an ambulatory MS patient from safely transferring for the
first 3 days after the dose adjustment but afterward provide best function. The next time an increase is needed, two smaller
increases may be more appropriate to ensure continued independent function. On the other hand, a patient with spinal cord
injury may experience relief of spasms within 1 hour of a 10% bolus of the daily dose on a previous occasion, but experience
no relief when this dose is repeated; in this case, further investigation of system function is in order. Knowing these details
contributes to safety, quality, function, and patient satisfaction. The nurse coordinator may be the healthcare provider patients receiving
ITB therapy visit most regularly. Therefore, ITB therapy nurses address not only direct effects and side effects of ITB but
also related issues such as changes in health, emotions, weather, and treatments that influence spasticity. It is important
to document not only tone, spasticity, and strength but also changes in prescription or over-the-counter medications or alternative
and herbal therapies. Traditional rehabilitative therapies as well as hippotherapy, hydrotherapy, and yoga may influence patient
function and should be documented. System changes that warrant evaluation for their effect on spasticity are listed in Table 3 . Ongoing assessment by consistent providers identifies these conditions
and guides dose adjustments and referral to other team members for treatment as indicated. This holistic approach facilitates
ITB therapy effectiveness with the lowest possible dose and contributes to best outcomes and patient satisfaction. Care by consistent healthcare providers and knowledge of a patient's ITB
therapy not only improves outcomes but also provides the best mechanism to continually monitor system function. Experienced
providers maintain an index of suspicion of system malfunction and develop a methodical process to identify and rule out causes
of loss of benefit. Each center's resources dictate its specific plan of action. During evaluation for system disruption,
the surgeon is an active participant, and radiologists are frequently introduced into the extended team. The role of the nurse
coordinator, surgeon, primary care providers, and emergency room department for each setting must be discussed, outlined,
and documented. The first line of contact varies by center; patients must know signs of acute withdrawal syndrome and overdose
as well as the appropriate person to call. Written guidelines for the patient and various points of patient contact for emergent
care are invaluable. Use of written protocols and standing orders ensure retention of institutional knowledge and consistency
as team members change. Catheter and infusion-system failure or overdosing is rare. However, because
either can be life threatening, early recognition is crucial to minimize risk. Both severe overdose and sudden withdrawal
can be identified, and treatment is described in a number of sources (Coffey et al., 2002; Gianino, York, & Paice, 1996;
Medtronic, 2002, 2005). Although not available at the time of the forum, the SynchroMed II clinical reference guide (Medtronic,
2004) and product monograph (Medtronic, 2005) review current treatment guidelines. In brief, overdosing symptoms are usually
related to human error in catheter volume or dosage programming. Review of the latest pump programming or manipulation of
the implanted system will identify the cause. For example, failure to aspirate the catheter contents before infusing contrast
through the catheter port is dangerous as it results in approximately 0.2 ml of baclofen rapidly infusing into the cerebrospinal
fluid and is likely to cause rapid, severe overdosing. Respiratory depression can result. On the other hand, sudden onset
of severe withdrawal symptoms of spasms, spasticity, irritability, and pruritus is likely to be caused by either a missed
refill date or pump system failure. After an empty pump reservoir has been ruled out, this situation requires immediate attention
to identify the specific system malfunction and appropriate surgical repair. Identification of the reason for gradual loss of therapeutic effect is
more challenging. Causes include disease progression, a new or recurring condition, or a change in prescribed or over-the-counter
treatment. Patient evaluation identifies disease progression or a comorbidity causing irritation such as urinary tract infection
or skin breakdown. Appropriate treatment of concurrent illness as well as a temporary rate increase should resolve the spasticity.
Addition or discontinuation of other agents may contribute to either high-dose effect or increased spasticity through drug
interactions. One example is the interferon injection used by some patients with MS, which may increase spasticity. Identifying
this pattern and treating it with oral baclofen is usually sufficient. Evaluation of ITB dosing should be considered if no change in health status
or treatments is identified. Review of response to past rate adjustments, specific patterns and activity surrounding the return
of symptoms, and history of goal achievement may indicate that a revision in total daily dose or dosing pattern is needed.
Rate increases are not unusual for patients with progressive diseases or during growth spurts in adolescents. The possibility
of drug tolerance exists (Nielson, Hansen, Sunde, & Christensen, 2002). An action for loss of benefit may include administration of an oral dose
of baclofen at home as part of phone-triage care. This may be particularly useful for patients who live far from the center,
in conjunction with the local primary care provider's evaluation of changes in general health status. Once the patient arrives
at the center, the effect of a programmed bolus dose on signs and symptoms provides useful information and can be done while
awaiting initial X rays. If these actions provide relief, further dose titration may be all that is needed. Intensity and
time to positive effect of the bolus can provide useful information to determine a treatment plan. A short-lived effect or
no effect at all from the bolus dose is indicative of catheter or pump system failure. A bolus infusion may relieve symptoms
even if there is a microtear, positional leak, or mass at the catheter tip. Catheter tip masses and arachnoiditis are known
to occur with intrathecal pain management; they have not been reported with intrathecal baclofen but can be considered. System-related loss of benefit is usually catheter related and requires
careful radiological evaluation of the pump, catheter, and spinal canal. Methods to evaluate the implanted system are reviewed
in a number of sources (Dickerman & Schneider, 2002; Hicks, Kaiff, Barzenor, Rahmat, & Kelly, 1989; Le Breton et al.,
2001; Medtronic, 2002, 2004; O'Connell et al., 2004; Rosensen, Ali, Fordham, & Penn, 1990) and are beyond the scope of
this article. Specific steps or order of tests depends on resources and varies among centers. If an X ray is not readily available,
catheter port aspiration may be the first tool to rule out catheter dislodgement or fracture. A small leak or microtear is
difficult to determine and verification may not be possible, even with nuclear medicine studies. Signs of inconsistent drug
delivery or fluctuation in tone may be caused by subdural catheter tip placement, arachnoiditis, or a positional catheter
leak. Positive response to a screening trial with no notable benefit from continuous infusion after weeks of therapy also
warrants investigation of system function. If no specific radiological results are found, clinical judgment may lead to replacement
of a potentially failed catheter based on symptoms alone. One other potential complication contributing to loss of benefit may be
a cerebrospinal fluid leak within the first weeks of surgery. This can be differentiated from a seroma by a history of headache
(especially on arising) fluctuant collection of fluid at the pump or back incision, and lack of ITB therapy benefit. Fluid
aspirated from the pump pocket will contain beta-2 transferrin, unique to cerebrospinal fluid, and confirm a leak rather than
a seroma. Seromas are rare and tend to appear when a pump is replaced. The prevailing theory is that the amount of scar tissue
and the extent of pocket revision are factors in the development of a seroma. For those with extensive scar tissue or significant
pocket revision, seromas may be prevented by use of an abdominal binder after pump replacement and decreased activity level
dependent on the patient's condition. During routine refill and dose adjustment visits, ongoing evaluation of
ITB therapy and the implanted system includes documentation of refill volume, actual reservoir volume compared to expected
volume, rate changes, and dose effect. Prevention of serious adverse events is dependent on education of the patient, family,
and team members. Such education can lead to early recognition of complications and initiation of appropriate skilled treatment. In addition to a coordinated and collaborative clinical team, practice
resources contribute to an efficient and profitable ITB therapy management program that provides quality care. These include
leadership, adequate facilities, and support staff. Designated team leaders are champions who maintain positive reputations
with administrators and the clinician referral base. They represent the team and acquire required resources. Ideally, team
members such as surgeons, therapists, and radiologists are geographically and administratively close to increase efficiency
of the clinicians and convenience for patients and to allow for best reimbursement, which adds to program success. Long-term management of ITB therapy usually occurs in a physician's office
or outpatient clinic. An appropriate facility includes space for patient office visits, access to procedures, and equipment
to troubleshoot potential complications. Patients requiring ITB therapy have various functional levels. They arrive at the
clinic for pump refills and programming adjustments either ambulating or with assistive devices such as seating systems. A
handicapped-accessible clinic setting with large hallways and doorways is mandatory. Exam rooms should accommodate not only
the clinical team and patient but also the 2–3 caregivers who may accompany the patient. Support staff enhance the efficiency of the clinical team. A reimbursement
contact assists in appropriate billing, diligently tracks best procedural and visit codes, and explores reimbursement strategies.
A mechanism to purchase specific supplies such as catheter access kits and refill kits should be identified. Although patients should be encouraged to be accountable for scheduling
refill appointments, support staff can oversee refill schedules to avoid low dosages or withdrawal. Information regarding
the risks of refill delays must be communicated not only to the patient but also to those responsible for scheduling the patient's
return visits. Scheduling refill visits several days before the anticipated low-volume-reservoir alarm date should be considered,
especially if weather or distance may be a problem. When rate adjustments occur between routine refills, the appropriateness
of prescheduled refill appointments should be verified; the dosage change will alter refill timing. Many centers develop a
patient database to ease scheduling. Patients requiring frequent visits appreciate extended clinic hours, especially patients
who attend school or work a regular workday. These accommodations diminish burden and encourage compliance. Support staff or clinicians responsible for refill scheduling can enhance
time management by allowing approximately 30 minutes for routine refills and allowing morning work-in time to evaluate patients
with potential complications. ITB therapy can be of tremendous benefit for patients with severe spasticity
that is unresponsive to more conservative treatment options. However, it is not simply a procedure but a comprehensive program
provided by a multidisciplinary team of healthcare practitioners. Nurses, particularly advanced practice nurses, are ideal
to coordinate long-term management of patients receiving this therapy. Patient satisfaction and overall outcomes are enhanced
when each stage of the therapy is managed with an emphasis on clear communication of the goals of treatment and a strong focus
on patient and family education. The treating team must include rehabilitation therapy disciplines to maximize the patient's
response to ITB therapy. Ongoing management should include individualized attention to dosing options and comprehensive evaluation
by a consistent team of providers. Adequate mechanisms must be in place to provide for appraisal and troubleshooting of the
pump and catheter system as needed, addressing of any pump-related emergency care, and problem solving as the patient's condition
or situation changes. The print version of this article was originally certified for CE credit.
For accreditation details, contact the publisher, American Association of Neuroscience Nurses (AANN), 4700 W. Lake Avenue,
Glenview, IL 60025-1485 Special thanks are given to Carolyn A. White. Support
for this article was provided by Medtronic, Inc. Questions or comments about this article may be directed to Barbara Ridley,
RN FNP, at 510/204-5259 or ridleyb@sutterhealth.org .
I have PLS and have been experiencing life changing symptoms for about
2 years. I haven't shared much of my personal experiences in this forum. I've been selfishly gathering strength from the experiences
shared by others. In those past months I went from a slight gimpy gait when I jogged to falling over once in awhile, to using
a cane and then a walker around the house and a wheelchair when out as the falls became harder with more serious injury. I
walk so slowly now that it's impractical to be out with others and expect to cover any real distance if I use the walker. |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
All health-related
material is provided for information purposes only and does not necessarily represent endorsement by or an official position
of the author of this website. Advice on the treatment or care of an individual patient should be obtained
through consultation with a physician who has examined that patient or is familiar with that patient's medical history.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||


 The only part that shows is the top part, where the markings are. I remember the horror I felt seeing that long tube
sticking out of me after surgery. Now I knew I was sick. Like having a wheelchair strapped to my ass wasn't a
clear indication? But the PEG was different, harder emotionally to accept. I knew I needed it for water (hydration)
but resisted using the PEG for nutrition. I think if I'd had the Mic-Key style it would have been emotionally easier
to use.
The only part that shows is the top part, where the markings are. I remember the horror I felt seeing that long tube
sticking out of me after surgery. Now I knew I was sick. Like having a wheelchair strapped to my ass wasn't a
clear indication? But the PEG was different, harder emotionally to accept. I knew I needed it for water (hydration)
but resisted using the PEG for nutrition. I think if I'd had the Mic-Key style it would have been emotionally easier
to use.